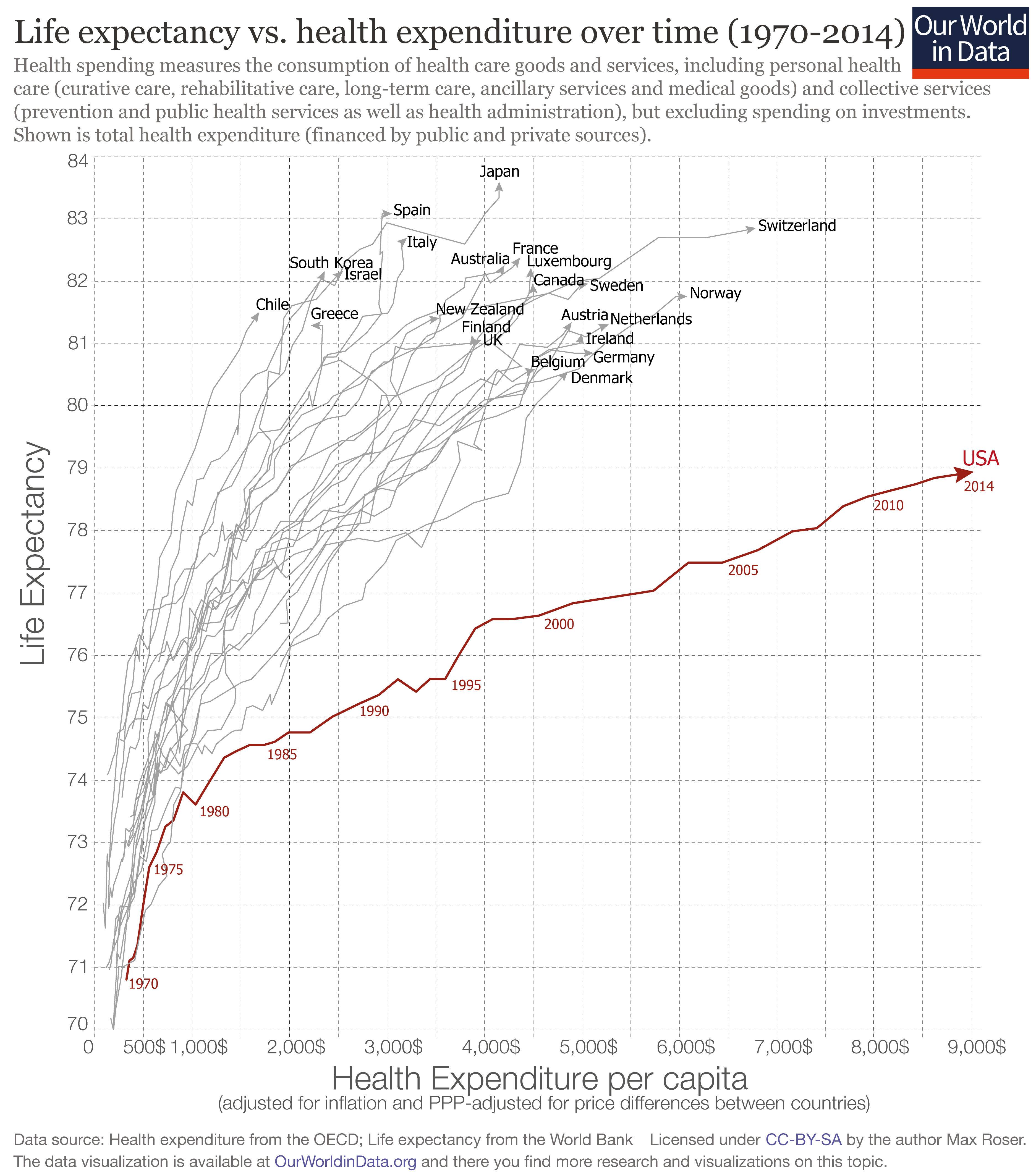
The figure shows patterns of health spending and life expectancy in various high-income countries from 1970 to 2014. Around 1970, all the countries are down in the bottom left corner of the figure. Over time, both health spending and life expectancy rise everywhere. But as you can see, the US is an outlier. Over the last 45 years or so, US health spending rises to much higher levels than in other countries, while the gains in life expectancy have been much more modest.
The US political arguments over health care have pretty much ignored this pattern: that is, we argue back and forth over costs and coverage of US health insurance, but we spend relatively little time thinking about what public policy steps would most improve health.
The March/April 2017 issue of the Rand Review has a short essay by Doug Irving, "What Are the Social Determinants of Health?" (pp. 6-10), which describes some research in this area. One can make a plausible case that the US could improve its life expectancy and health levels with a tradeoff of less social spending on health care, but more social spending on housing, food, education, drug rehabilitation, and safe neighborhoods. Irving writes:
"Where people live, what kinds of educational opportunities they have access to—these all seem to have strong effects on health,” said Kathryn Pitkin Derose, a senior policy researcher at RAND. ... She uses a simile that has become common in public-health circles to explain that need for a broader view of health care. The current system, she says, is like a lifeguard standing on the banks of a rushing river, always jumping in to rescue people at the last moment as they struggle in the water. What is needed, she says, is a new perspective—a new focus on what causes so many people to fall into the river in the first place, and on addressing those problems before more people follow. “You have to go upstream,” she says, “to see what's really affecting people's health.”It's a question of opportunity cost: when the government devotes so much of its spending and so much of its support for those with low incomes to health care spending, other possibilities for social spending are inevitably constricted.
For a previous post arguing that a substantial share of health spending is wasted, both in the US and around the world, see "Wasteful Health Care Spending" (February 23, 2017).
Homage: I ran across this figure at Mark Thoma's ever-useful "Economist's View" blog.